
The concept of health literacy has become increasingly popular. But what actually is it, and how is it relevant to health and equity?
Our team began investigating these questions nearly two decades ago. The first measures of health literacy in the 1990s focused on functional literacy and numeracy in health contexts, the measurement of which no longer fully captures modern multidimensional health literacy concepts. Importantly, measurement of only health-related literacy may lead to discrimination and stigmatisation and may even increase health inequities because broader health literacy factors are not considered. While literacy is required (e.g., to read medication labels and health promotion materials), there are other skills and resources that individuals and families need to access, understand, appraise, remember, and use health information and services.
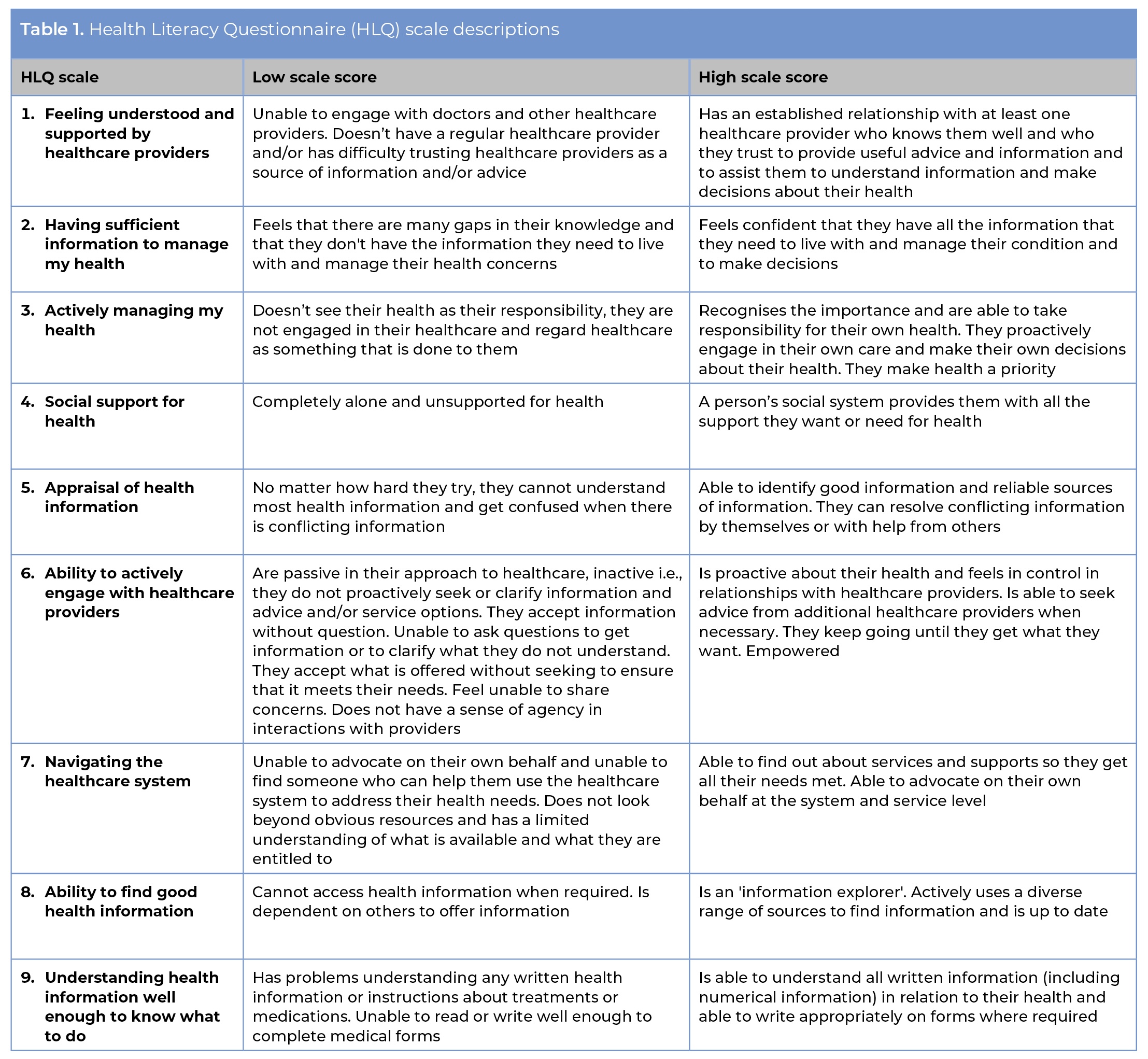
To advance health literacy measurement to equitably support health-related decisions and behaviours, our research team explored what people actually need. We asked community members this question: Thinking about your experiences in trying to look after your health (or the health of your family), what abilities does a person need to have in order to get and use all of the information they need? When combined with input from healthcare providers and policy makers, health literacy was found to be more than just literacy. Through extensive consultation and testing, a nine-dimension health literacy construct was confirmed (table 1) and now comprises the Health Literacy Questionnaire (HLQ), which has demonstrated strong psychometric properties1. The nine HLQ scales are scored separately (i.e., no single overall score) to reveal profiles of health literacy strengths (scales with higher scores) and challenges (lower scores), with each scale score being relative to the other eight scale scores in the profile.
After presenting these nine dimensions to experienced primary healthcare physicians, we received strong confirmation that these dimensions reflect struggles many of their patients may have daily. Further input from across sectors confirmed that the HLQ dimensions are meaningful and useful to clinicians, giving us impetus to push this field forward.
Health literacy is woven through the community fabric
Our research demonstrates that health literacy is embedded in the relationships, values, and knowledge in families, communities, organisations, and nations2. It is found in people’s daily practices, routines, cultures, community connections, workplaces, and environments. To understand how to develop health literacy, we need to understand people’s strengths and challenges in their contexts. We need to learn about the “community fabric”3 to find what works, for whom, under what circumstances, and why. Such learning means engaging – authentically engaging – with community, especially with those who are likely to be left behind from receiving the care they need. These are usually the people for whom the social determinants of health make circumstances difficult for patients to get and receive care, and for clinicians to deliver equitable care.
Our work in primary care and community health aims to improve outcomes for community members and to improve how healthcare providers can do their daily work. Our conceptualisation of health literacy seeks to provide researchers and health organisations with key information about community needs and what health services can do to improve health outcomes. To achieve this, we use health literacy data to uncover mechanisms that lead to health inequities, and to generate actions that reduce the burden on clinicians and on community members so they can seek and receive the care they need.
Measurement to inform intervention development
The value of measurement with the HLQ is the nine-scale health literacy profiles for needs assessment. In clinical research and epidemiology, health literacy measurement frequently generates single overall scores and population averages. These are of little use for clinical practice and community care where clinicians are treating individual patients who have their own personal strengths and challenges for managing their health. To treat each person as an average is anathema to good clinical practice. Moving beyond averages, we use cluster analysis to reveal different score patterns for different groups of people within a population4. Groups of people with multiple health literacy challenges may not benefit from, or even engage in, usual care or one-size-fits-all health promotion initiatives, which puts them at risk of being left behind. Even well-intentioned community care and health promotion will reach only some people (i.e., people who are mostly well, with resources, and who are able or are supported to manage their health) while excluding those most in need (i.e., people with multiple health conditions, without resources or support). We need different interventions to suit the situations of different groups of people.
How do we know what will best suit different groups of people?
We ask them! And co-design with them! Community members have personal knowledge and expertise in accessing and using health information and services, so let’s build on what they know – on their strengths – and what they can share with others. Some community members, despite having little education and few resources, can have exceptionally positive behaviours and are efficient users of health services. Some individuals can be illiterate and have difficulty appraising health information or knowing what to do for their health, yet they have social support or a trusted clinician to explain information and treatments. Every day, clinicians recognise and overcome the health literacy challenges of their patients. Co-design enables the tacit expertise of community members and clinicians to inform and improve the quality of, and reduce inequities in, the delivery of health services. However, co-design does require a different way of thinking about health service reform.
Co-designing systematically for health and equity outcomes
Co-design is a way of designing with people, not for people5. Power must be given away by those who usually hold it. Shared power means relationships are prioritised. Those who usually do not hold power must learn that their voice is of value and will be heard. It can be challenging to incorporate the perspectives of many stakeholders, so respect and patience are needed.
A requirement for building co-designed initiatives is to be comfortable with uncertainty. Co-design elevates the lived experiences of community members and clinicians to see what can be learned about how services can be improved, which means the outcomes of a co-design initiative are uncertain at the beginning. At the start, the interventions to be implemented are unknown because they are built from stakeholder experiences – including community members and clinicians – rather than built from what is known in the literature or from a known intervention that has been implemented elsewhere. Using a strengths-based approach (see also assets-based model)6, co-design helps to reduce research waste and the implementation of inequitable one-size-fits-all health interventions.
A breakthrough in co-design research is the Optimising Health Literacy and Access (Ophelia) process, a systematic participatory co-design methodology endorsed by the World Health Organization (WHO)7,8 and widely used in Europe. Ophelia provides a three-phase, step-by-step co-design process that allows for flexibility in methods, depending on contextual factors. A health literacy needs assessment is conducted with the HLQ or eHealth Literacy Questionnaire (eHLQ)9 to inform the development of interventions that are appropriate, meaningful and useful to communities and health services. The European Union Joint Action on Cardiovascular Diseases (CVD) and Diabetes (JACARDI) Work Package 6 (WP6) on Health Literacy10 is applying the Ophelia process. There are four Spanish WP6 projects:
- Promotion of health literacy about CVD and diabetes through a massive open online course (MOOC) (Cantabria)
- Health literacy of adolescents (Basque Country)
- Health literacy of people who have suffered ischaemic stroke (Aragon)
- Health literacy on nutrition and physical activity in health-promoting schools (Aragon)
The strengths-based co-design approach of the Ophelia process applies the science of intervention development to transform needs assessment data into practical and tangible initiatives to generate health and equity outcomes for diverse community members. Ophelia projects co-design community-developed interventions that improve the health literacy responsiveness of services to meet the needs of the communities they serve. The well-recorded insights of all stakeholders, including from primary healthcare providers, is fundamental to the success of Ophelia projects to build and implement needed and wanted innovations.
RECOMMENDED CITATION:
Hawkins M, Osborne RH. Health literacy development: co-design for health and equity outcomes. Comunidad. 27;(2):43-46. DOI: 10.55783/comunidad.270202
